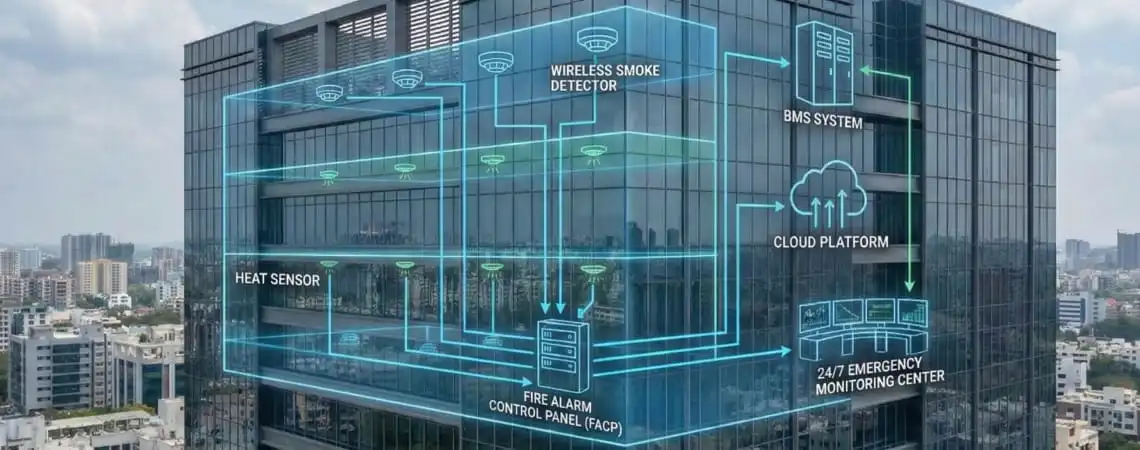
AIoT (Artificial Intelligence of Things) fire safety combines IoT sensor networks with AI-powered analytics to detect fires faster, reduce false alarms, and automate emergency responses. Unlike traditional fire alarms that only sound alerts, AIoT systems analyze multiple data streams in real-time and automatically control building systems like HVAC, elevators, and access controls to contain fires and protect occupants.
For hospitals where patients cannot evacuate independently, this automated response happens in seconds—not minutes—making the critical difference between containment and catastrophe.

Between 2011 and 2024, approximately 180 patients including several newborns died in 13 massive fire incidents across hospitals in India. The pattern is consistent: emergency exits locked, fire extinguishers non-functional, and response times too slow.
In November 2024, a fire broke out in the NICU of Maharani Laxmi Bai Medical College in Jhansi, killing at least 10 newborns from burns and suffocation, allegedly caused by an electrical short circuit. Families reported locked emergency exits and non-functional fire extinguishers.
These tragedies share common failures:
According to NFPA Standard 1710, fire departments aim for an 80-second turnout time and 240-second travel time, totaling 320 seconds (5 minutes 20 seconds) response time for structure fires. But this measures only emergency responder arrival—not the critical minutes before notification.
Research shows that with alarm bells alone, evacuation can take 8 minutes 15 seconds to begin, compared to just 1 minute 15 seconds when staff marshals provide direct guidance.
Traditional Fire Alarm Response Chain:

Total: 2-3 minutes minimum
For immobile hospital patients, these delays prove fatal. Smoke inhalation, not burns, is the primary cause of death in fires.
AIoT systems monitor multiple parameters simultaneously rather than relying on single-threshold detection:
This contextual intelligence enables AIoT systems to distinguish between normal hospital operations (surgical cautery, sterilization processes) and genuine fire threats, dramatically reducing false alarms while improving genuine threat detection.

AIoT systems process sensor data locally at the network edge rather than transmitting to centralized control panels. When combustion signatures appear, the detection apparatus itself initiates pre-programmed response sequences without requiring human interpretation.
This 67-80% reduction in response time directly determines patient survival outcomes when smoke fills an ICU or NICU.
Upon detecting fire signatures, AIoT systems automatically execute coordinated responses across all building infrastructure:
Smoke control systems activate automatically when fire alarms or sprinkler flow sensors detect incidents, with control panels switching HVAC operation from normal mode to smoke control mode within seconds.

NFIRE represents the next generation of AIoT-enabled fire safety specifically designed for healthcare environments where traditional systems fall short.
In operational facilities like hospitals, wireless systems can be installed with 80% less disruption to daily activities compared to wired alternatives.
NFIRE’s wireless topology enables:
Traditional addressable systems requiring extensive wiring can take 4-8 weeks to install and necessitate closing hospital wings—an untenable disruption for operational healthcare facilities.
NFIRE’s multi-parameter algorithmic processing addresses the historically vexing tradeoff between sensitivity and false alarm rates. The system analyzes:
This contextual discrimination achieves 90% false alarm reduction compared to traditional single-threshold systems, while detecting real fires earlier—often at smoldering stages before visible smoke development.
For hospital operations, this means:
NFIRE integrates seamlessly with critical hospital infrastructure through industry-standard protocols:
HVAC Systems: Automated zone shutdown, smoke damper control, corridor pressurization via BACnet or Modbus integration
Emergency Lighting: Instant activation of egress guidance and emergency illumination in affected zones
Access Control: Coordinated unlocking of egress routes and lockdown of hazard zones through integration with card access and electromagnetic lock systems
Elevator Controls: Automatic recall and firefighter service mode activation
Sprinkler Systems: Coordinated activation sequencing to prevent water damage in non-fire zones
Smoke Exhaust: Automated activation of smoke evacuation fans in designated zones
Unlike traditional fire panels that merely send notification signals, NFIRE executes direct control over building infrastructure to create survivable conditions automatically.
Smart fire systems provide real-time, remote access to fire system status and events, as well as detailed analytics and reports, helping managers quickly identify and address potential issues.
NFIRE provides:
NFIRE recognizes distinct risk profiles of different hospital areas:
Intensive Care Units (ICUs): Hypersensitive multi-parameter monitoring accounting for medical equipment while detecting genuine threats instantly
Operating Theatres: Specialized algorithms distinguishing surgical equipment signatures from fire hazards
Neonatal ICUs: Highest sensitivity settings with automated response protecting immobile newborns
General Wards: Balanced detection appropriate for patient rest areas
Pharmaceutical Storage: Enhanced thermal and electrical monitoring for high-risk medication areas
Utility Spaces: Robust detection for equipment rooms and mechanical areas
Each zone receives customized monitoring parameters, threat assessment algorithms, and automated response protocols calibrated to specific occupancy patterns and operational requirements.
Conventional fire alarm systems are fundamentally designed to notify human operators, not execute protective actions autonomously. This alert-based philosophy delegates all subsequent decision-making to personnel who may lack:
Traditional systems typically employ fixed threshold parameters that trigger alarms when readings exceed predetermined values. A smoke detector activates at X particles per cubic meter; a heat detector triggers at Y degrees Celsius.
This rigid calibration demonstrates profound inadequacy within hospital environments where operational context determines appropriate response:
Traditional systems lack contextual intelligence to distinguish between benign operational variations and authentic conflagration threats.
Most critically, conventional fire alarm infrastructure operates in complete isolation from building systems that determine fire propagation velocity and occupant survivability:
Even the most sophisticated traditional fire panel has no control over:
This systemic fragmentation ensures that even when fires are detected within seconds, building infrastructure continues operating in modes that inadvertently facilitate disaster progression.
In 2011, 94 people including 90 patients died at AMRI Hospital in Kolkata when inflammable material stored illegally in an underground car park caught fire and spread through air conditioner ducts.
The fire spread through HVAC systems because they continued operating in normal mode. Traditional fire alarms detected the fire—but could not automatically isolate ventilation zones or prevent smoke circulation.
NFPA 101 Life Safety Code Section 19.7.7.1 establishes performance requirements for smoke control systems in healthcare facilities.
Starting with the 2022 edition of Joint Commission Standards, retesting of smoke control systems in existing accredited hospitals became mandatory.
The International Building Code Section 909 requires smoke control systems for atriums open to two or more stories in hospitals and nursing homes.
NBC (National Building Code) 2016 Part 4 contains detailed provisions for fire and life safety, including:
The Ministry of Health and Family Welfare mandated No-Objection Certificates and quarterly fire audits for all hospitals in 2020 following COVID-19 hospital fires.
Healthcare facilities may use private operating mode fire alarms in ICUs, operating theaters, and hospital nurseries, where traditional building-wide alarms could adversely affect patient care.
NFIRE supports both private and public mode configurations, allowing:

Traditional Wired System Installation:
NFIRE Wireless Installation:
Cost Considerations
While AIoT fire protection systems require initial investment, they deliver measurable ROI:
Direct Cost Savings:
Risk Mitigation Value:
Operational Benefits:
When a smoke detector activates at 3:00 AM in your ICU, what happens in the first 60 seconds?
If the answer is “an alarm sounds and security is notified,” you have a notification system, not a protection system. Genuine safety requires automated action—HVAC isolation, smoke damper closure, elevator recall, egress unlocking—occurring within that first minute, independent of human intervention.
Evaluate whether your fire safety architecture specifically addresses:
During fire detection:
If any answer is “no” or “it depends on staff action,” your building infrastructure will continue operating in modes that facilitate smoke propagation even after fire detection.
Hospital fire incidents demonstrate that conventional approaches predicated on manual intervention and isolated system operation cannot safeguard non-ambulatory patient populations during the seconds and minutes determining survival outcomes.
True resilience emerges from systems capable of:
This is the promise of AIoT-driven fire safety platforms like NFIRE: not merely faster alarms or more sensitive detectors, but fundamentally reimagined protection architecture where intelligence resides in the system itself.
Hospital leadership should frame fire safety enhancements as clinical risk mitigation investments equivalent to infection control infrastructure or medication safety systems. When fire occurs in an ICU housing ventilated patients, the threat is as immediate as any medical emergency.
According to India’s National Crime Records Bureau, the country recorded 7,566 fire-related accidents in 2022, resulting in 7,435 deaths, with electrical faults remaining the most frequent ignition source.
Every hospital operating with traditional alert-based fire safety systems remains vulnerable to the pattern that has played out repeatedly: electrical anomalies accumulating, warnings dismissed, alarms sounding too late, smoke spreading too quickly, and immobile patients unable to escape.
The question confronting healthcare leadership is not whether to upgrade fire safety systems, but when—and whether that decision will be made proactively or reactively, before or after the next incident.
1. Schedule Comprehensive Fire Safety Assessment
2. Request NFIRE AIoT System Demonstration
3. Evaluate Current System Response Times
4. Review Integration Capabilities
5. Plan Wireless Retrofit Strategy
Traditional fire alarms detect fires and sound alerts requiring human response. AIoT fire safety systems use artificial intelligence and IoT sensors to detect fires, analyze threats contextually, and automatically control building systems (HVAC, elevators, access controls) to contain fires—all within 60 seconds without human intervention.
Traditional systems require 2-3 minutes from detection to meaningful human-directed response. AIoT systems like NFIRE execute protective actions within 60 seconds—a 67-80% reduction in response time that is critical when smoke fills an ICU.
Hospitals house immobile patients who cannot evacuate independently: ventilated patients on life support, sedated individuals, newborns in incubators, and post-surgical patients. Traditional fire safety assumes occupant mobility and self-preservation capability, which does not apply to healthcare environments.
NFIRE analyzes multiple parameters simultaneously (particulate density, thermal rate-of-rise, electrical anomalies, airflow patterns) and learns normal operational baselines for each zone. This contextual intelligence distinguishes between normal hospital operations (surgical equipment, sterilization) and genuine fire threats.
Yes. NFIRE’s wireless architecture enables 7-10 day installation without invasive construction, ceiling demolition, or operational disruption. Traditional wired systems require 7-11 weeks and often necessitate closing hospital sections.
NFIRE automatically controls HVAC systems (zone isolation, smoke damper closure, corridor pressurization), elevators (recall to ground level, firefighter mode), access controls (egress unlocking, hazard zone lockdown), emergency lighting (directional evacuation guidance), and sprinkler systems (coordinated activation).
Yes. NFIRE complies with NBC 2016 fire safety requirements while exceeding minimum standards through intelligent automation. The system also meets NFPA standards and Joint Commission requirements for healthcare fire safety.
Edge computing processes sensor data locally at the network edge rather than transmitting to centralized control panels. This eliminates transmission delays and enables the detection apparatus itself to initiate protective responses within 5-15 seconds of threat identification.
Ready to upgrade from notification to protection? Contact us to schedule a NFIRE demonstration and comprehensive fire safety assessment for your healthcare facility.
NFIRE: When every second is clinical, fire protection cannot wait for human response.